Zuclopenthixol decanoate.
Zuclopenthixol decanoate 200 mg/ml.
Excipients/Inactive Ingredients: Medium-chain triglycerides.
Pharmacotherapeutic group: Neuroleptics, Antipsychotics - Thioxanthene derivative. ATC-code: N 05 AF 05.
Pharmacology: Pharmacodynamics: Mechanism of action: Zuclopenthixol is a neuroleptic of the thioxanthene group.
The antipsychotic effect of neuroleptics is related to their dopamine receptor-blocking effect but possibly also 5-HT (5-hydroxytryptamine) receptor blockade contributes.
In vitro, zuclopenthixol has high affinity for both dopamine D1 and D2 receptors, for α1-adrenoceptors and 5-HT2 receptors but no affinity for cholinergic muscarinic receptors. It has weak histamine (H1) receptor affinity and no α2-adrenoceptor-blocking activity. In vivo, the affinity for D2 binding sites dominates over the affinity for D1 receptors.
Zuclopenthixol has proven to be a potent neuroleptic in all the behavioural studies for neuroleptic (dopamine receptor-blocking) activity. Correlation is found between the in vivo test models, the affinity for dopamine D2 binding sites in vitro and the mean daily oral antipsychotic doses.
Like most other neuroleptics, zuclopenthixol increases the serum prolactin level in a dose-dependent manner.
Pharmacological studies have shown that zuclopenthixol decanoate in oil has extended antipsychotic activity and that the amount of drug needed to maintain a given effect over a prolonged period is substantially less with the modified-release preparation than with daily oral doses. Pharmacological studies also indicate that a prolonged antipsychotic effect can be clinically achieved with the modified-release preparation without obvious sedation. Furthermore, the risk of interaction with anaesthetic agents is expected to be low.
In clinical use, Clopixol Depot is intended for maintenance therapy of chronic psychotic patients.
Zuclopenthixol decanoate induces a transient dose-dependent sedation. However, sedation is not a problem if patients are switched from oral Clopixol or Clopixol Acuphase to maintenance therapy with Clopixol Depot. Patients rapidly develop tolerance to the non-specific sedative effect.
Clopixol Depot is particularly suitable for the treatment of psychotic patients who are agitated, restless, hostile and aggressive.
Clopixol Depot ensures continuous antipsychotic treatment and reduces the rate of recurrence due to non-compliance among patients receiving oral therapy.
Paediatric population: No data available.
Pharmacokinetics: Absorption: Intramuscular injection produces peak serum concentration (Tmax) after 3-7 days. With an estimated half-life of around 3 weeks (reflecting the modified-release), steady-state concentrations are achieved after approximately 3 months of repeated administration.
Distribution: The apparent volume of distribution (Vd)β is about 20 l/kg. The plasma protein binding is about 98-99%.
Biotransformation: The metabolism of zuclopenthixol proceeds along three main routes - sulfoxidation, side-chain N-dealkylation and glucuronic acid conjugation. The metabolites are devoid of psychopharmacological activity. Zuclopenthixol dominates over metabolites in brain and other tissues. Genetic polymorphism has been identified.
Elimination: The elimination half-life (T½ β) is about 20 hours and the mean systemic clearance (Cls) is about 0.86 l/min.
Zuclopenthixol is excreted mainly with faeces, but also to some degree (about 10 %) with the urine. Only about 0.1 % of the dose is excreted unchanged with the urine, meaning that the drug load on the kidneys is negligible.
In nursing mothers, zuclopenthixol is excreted in small amounts with the breast milk. In steady state, the pre-dose mean ratio milk conc./serum conc. in women treated orally or with the decanoate form was about 0.29 or approximately 0.3.
Linearity: The pharmacokinetics is linear. The Cmin of zuclopenthixol is approximately 25 nmol/l at steady state after a dose of 200 mg zuclopenthixol decanoate every 2 weeks.
Elderly patients: The pharmacokinetic parameters are widely independent of the patient's age.
Renal impairment: Not investigated. Based on the previously mentioned elimination data, however, it is reasonable to assume that renal impairment would not affect serum levels of zuclopenthixol to any major degree.
Hepatic impairment: Not investigated.
Toxicology: Preclinical safety data: Acute toxicity: Zuclopenthixol has low acute toxicity.
Chronic toxicity: In chronic toxicity studies, there were no findings of concern for the therapeutic use of zuclopenthixol.
Reproductive toxicity: In a three-generation study in rats a delay in mating was noted. Once mated there was no effect on fertility. In an experiment where zuclopenthixol was administered via the diet, impaired mating performance and reduced fertility were noted.
Animal reproduction studies have not shown evidence of embryotoxic or teratogenic effects. In a peri/postnatal study in rats, dosages of 5 and 15 mg/kg/day resulted in an increase of stillbirths, reduced pup survival and delayed development of pups.
Maintenance treatment of schizophrenia and other psychoses, especially with symptoms such as hallucinations, delusions, thought disturbances, in combination with agitation, restlessness, hostility, and aggressiveness.
Posology: Adults: Dosage and interval between injections will be individually adjusted by the treating physician according to the condition of the patient. This in order to achieve a maximum suppression of psychotic symptoms with a minimum of side effects.
Zuclopenthixol decanoate 200mg/ml: In the maintenance treatment the dosage range would normally be 200-400mg (1-2ml) every second to fourth week.
A few patients may need higher doses or shorter intervals between doses.
Injection volumes exceeding 2 ml should be distributed between 2 injection sites.
When changing the medication from oral zuclopenthixol or zuclopenthixol acetate i.m. to maintenance treatment with zuclopenthixol decanoate the following guidelines should be used: 1) Change from oral zuclopenthixol to zuclopenthixol decanoate: x mg p.o. daily corresponds to 8x mg decanoate every 2 weeks; x mg p.o. daily corresponds to 16x mg decanoate every 4 weeks.
Oral zuclopenthixol should be continued during the first week after the first injection but with a reduced dose.
2) Change from zuclopenthixol acetate to zuclopenthixol decanoate: Concomitantly with the last injection of zuclopenthixol acetate (100 mg), 200-400mg (1-2ml) of zuclopenthixol decanoate 200mg/ml should be given intramuscularly and repeated every 2 weeks. Higher doses or shorted interval may be needed.
Zuclopenthixol acetate and zuclopenthixol decanoate can be mixed in a syringe and given as one injection (co-injection).
Patients being transferred from other depot preparations should receive a dose in the ratio of 200 mg zuclopenthixol decanoate equivalent to 25 mg fluphenazine decanoate, to 40 mg cis(Z)-flupentixol decanoate, or to 50 mg haloperidol decanoate.
Subsequent doses of zuclopenthixol decanoate and the interval between injections should be adjusted to the response of the patient.
Older patients: Older patients should receive dosages in the lower end of the dosage range.
Children: Clopixol Depot is not recommended for use in children due to lack of clinical experience.
Reduced renal function: Clopixol Depot can be given in usual doses to patients with reduced renal function.
Reduced liver function: Careful dosing and, if possible, a serum level determination is advisable.
Method of administration: Clopixol Depot is administered by intramuscular injection into the upper outer quadrant of the gluteal region. Injection volumes exceeding 2 ml should be distributed between 2 injection sites. Local tolerability is good.
Symptoms of overdose are unlikely to occur, owing to the administration route.
The highest orally administered dose of zuclopenthixol in clinical trials was 450 mg daily.
Symptoms: Somnolence, coma, extrapyramidal symptoms (movement disorders), convulsions, shock, hyperthermia/hypothermia.
ECG changes, QT prolongation, torsade de pointes, cardiac arrest and ventricular arrhythmias have been reported when zuclopenthixol has been taken in overdose concurrently with drugs known to affect the heart.
Treatment: Treatment is symptomatic and supportive. Measures to support the respiratory and cardiovascular systems should be instituted. Epinephrine (adrenaline) should not be used, as further lowering of blood pressure may result. Convulsions may be treated with diazepam and symptoms of movement disorders with biperiden.
Hypersensitivity to the active substance or to any of the excipients, listed in Description.
Circulatory collapse, depressed level of consciousness due to any cause (e.g. intoxication with alcohol, barbiturates or opiates), coma.
The possibility of development of neuroleptic malignant syndrome (hyperthermia, muscle rigidity, fluctuating consciousness, instability of the autonomous nervous system, increased serum creatine phosphokinase levels) exists with any neuroleptic. The risk is possibly greater with the more potent agents.
Patients with pre-existing organic brain syndrome, mental retardation and opiate/alcohol abuse are over-represented among fatal cases.
Treatment: Discontinuation of the neuroleptic. Symptomatic treatment and use of general supportive measures. Dantrolene and bromocriptine may be helpful.
Symptoms may persist for more than a week after oral neuroleptics are discontinued and somewhat longer when associated with the depot forms of the drugs (modified-release formulations).
Like other neuroleptics, zuclopenthixol should be used with caution in patients with organic brain syndrome, convulsions, diabetes and advanced hepatic or severe renal disease.
As described for other psychotropics, zuclopenthixol may modify insulin and glucose responses calling for adjustment of the antidiabetic therapy in diabetic patients.
Patients on long-term therapy, particularly on high doses, should be monitored carefully and evaluated periodically to decide whether the maintenance dosage can be lowered.
As with other drugs belonging to the therapeutic class of antipsychotics, zuclopenthixol may cause QT prolongation. Persistently prolonged QT intervals may increase the risk of malignant arrhythmias. Therefore, zuclopenthixol should be used with caution in susceptible individuals (with hypokalemia, hypomagnesemia or genetic predisposition to arrhythmia) and in patients with a history of cardiovascular disorders, e.g. QT prolongation, significant bradycardia (<50 beats per minute), a recent acute myocardial infarction, uncompensated heart failure, or cardiac arrhythmia.
Concomitant treatment with other antipsychotics should be avoided (see Interactions).
Cases of venous thromboembolism (VTE) have been reported with antipsychotic drugs. Since patients treated with antipsychotics often present with acquired risk factors for VTE, all possible risk factors for VTE should be identified before and during treatment with zuclopenthixol and preventive measures undertaken.
Leukopenia, neutropenia and agranulocytosis have been reported with antipsychotics, including zuclopenthixol decanoate.
Long-acting depot antipsychotics should be used with caution in combination with other medicines known to have a myelosuppressive potential, as these cannot rapidly be removed from the body in conditions where this may be required.
Effects on ability to drive and use machines: Clopixol Depot has a sedative effect which has minor or moderate influence on ability to drive and use machines. Patients who are prescribed psychotropic medication may be expected to have some impairment in general attention and concentration and should be cautioned about their ability to drive or operate machinery.
Use in the Elderly: Cerebrovascular: Zuclopenthixol should be used with caution in patients with risk factors for stroke.
An approximately 3-fold increased risk of cerebrovascular adverse events has been seen in randomised placebo-controlled clinical trials in the dementia population with some atypical antipsychotics. The mechanism for this increased risk is not known. An increased risk cannot be excluded for other antipsychotics or other patient populations.
Increased Mortality in Elderly people with Dementia: Data from two large observational studies showed that elderly people with dementia who are treated with antipsychotics are at a small increased risk of death compared with those who are not treated. There are insufficient data to give a firm estimate of the precise magnitude of the risk and the cause of the increased risk is not known.
Zuclopenthixol is not licensed for the treatment of dementia-related behavioural disturbances.
Pregnancy: Zuclopenthixol should not be administered during pregnancy unless the expected benefit to the patient outweighs the theoretical risk to the foetus.
Neonates exposed to antipsychotics (including zuclopenthixol) during the third trimester of pregnancy are at risk of adverse reactions including extrapyramidal and/or withdrawal symptoms that may vary in severity and duration following delivery. There have been reports of agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress, or feeding disorder. Consequently, newborns should be monitored carefully.
Animal studies have shown reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Lactation: Breast-feeding can be continued during zuclopenthixol therapy if considered of clinical importance, but observation of the infant is recommended, particularly in the first 4 weeks after birth.
As zuclopenthixol is found in breast milk in low concentrations, it is not likely to affect the infant when therapeutic doses are used. The dose ingested by the infant is less than 1% of the weight-related daily maternal dose (in mg/kg) (see Pharmacology: Pharmacokinetics under Actions).
Fertility: In humans, adverse events such as hyperprolactinaemia, galactorrhoea, amenorrhoea, erectile dysfunction and ejaculation failure have been reported (see Adverse Reactions). These events may have a negative impact on female and/or male sexual function and fertility.
If clinically significant hyperprolactinaemia, galactorrhoea, amenorrhoea or sexual dysfunction occur, a dose reduction (if possible) or discontinuation should be considered. The effects are reversible on discontinuation.
Administration of zuclopenthixol to male and female rats were associated with a slightly delay in mating. In an experiment where zuclopenthixol was administered via the diet, impaired mating performance and reduced conception rate was noted.
The most common undesirable effects are dry mouth, somnolence, akathisia, hyperkinesia and hypokinesia, which may occur in more than 10% of treated patients.
Summary of the safety profile: The undesirable effects are, for the majority, dose-dependent. The frequency and severity are most pronounced in the early phase of treatment and decline during continued treatment.
Extrapyramidal reactions may occur, especially in the early phase of treatment. In most cases, these side effects can be satisfactorily controlled by reduction of dosage and/or use of antiparkinsonian drugs. The routine prophylactic use of antiparkinsonian drugs is not recommended. Antiparkinsonian drugs do not alleviate tardive dyskinesia and may aggravate them. Reduction in dosage or, if possible, discontinuation of zuclopenthixol therapy is recommended. In persistent akathisia, a benzodiazepine or propranolol may be beneficial.
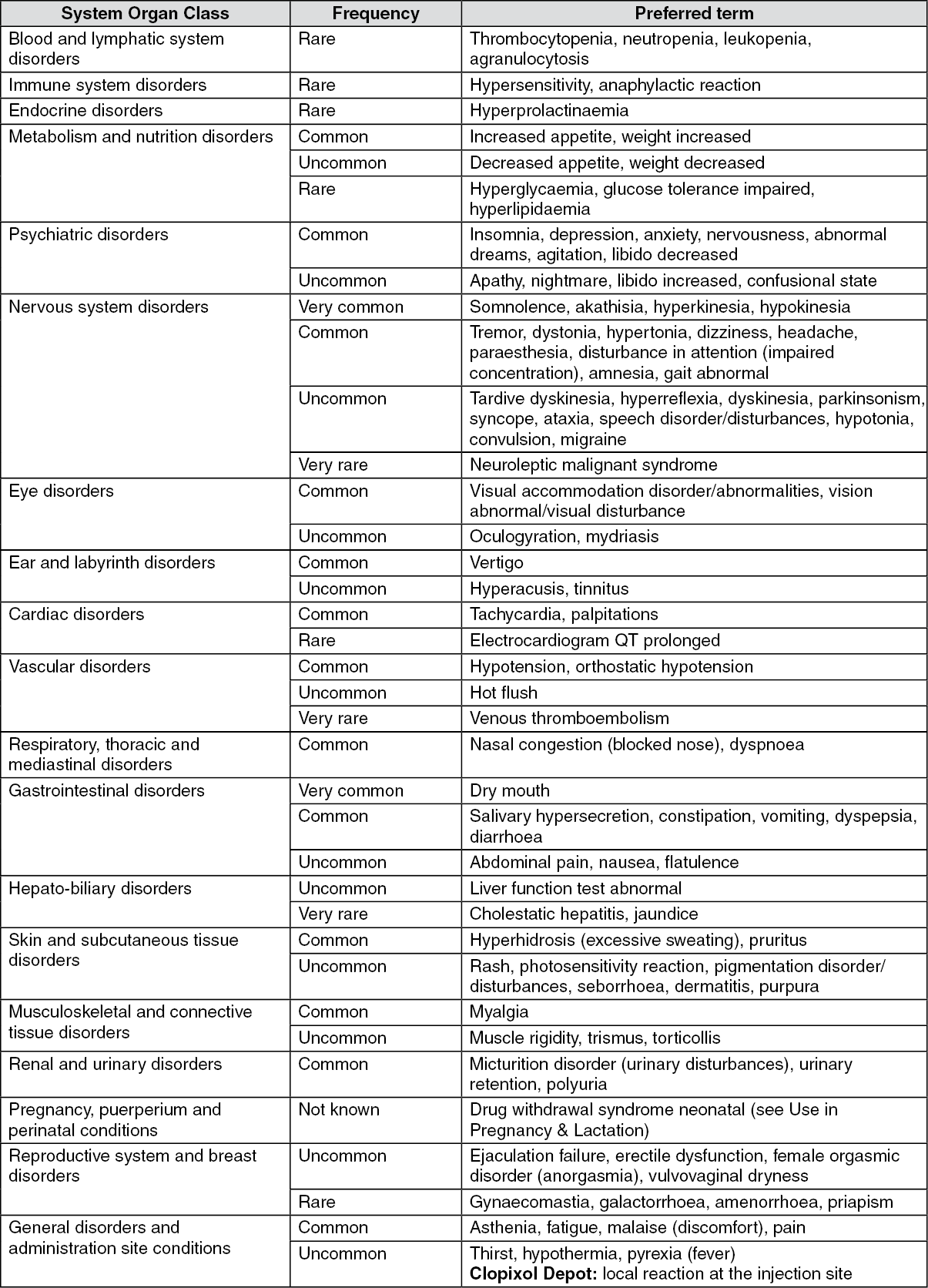
Tabulated list of adverse reactions: Frequencies are taken from the literature and spontaneous reporting. Frequencies are defined as: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10000 to <1/1000), very rare (<1/10000), or not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions:
Click on icon to see table/diagram/image
Description of selected adverse reactions: As with other drugs belonging to the therapeutic class of antipsychotics, rare cases of QT prolongation, ventricular arrhythmias (ventricular fibrillation and ventricular tachycardia), Torsade de Pointes, cardiac arrest and sudden unexplained death have been reported for zuclopenthixol (see Precautions).
Abrupt discontinuation of zuclopenthixol may be accompanied by withdrawal symptoms. The most common symptoms are nausea, vomiting, anorexia, diarrhoea, rhinorrhoea, sweating, myalgias, paraesthesias, insomnia, restlessness, anxiety, and agitation. Patients may also experience vertigo/dizziness, alternate feelings of warmth and coldness (hot and cold flashes), and tremor. Symptoms generally begin within 1 to 4 days of withdrawal and abate within 7 to 14 days or in 1 to 2 weeks.
Combinations requiring precautions for use: Zuclopenthixol may enhance/potentiate the sedative effect of alcohol and the effects of barbiturates and other CNS depressants.
Neuroleptics may increase or reduce the effect of antihypertensive drugs. The antihypertensive effect of guanethidine and similar acting compounds is reduced.
Concomitant use of neuroleptics and lithium increases the risk of neurotoxicity.
Tricyclic antidepressants and neuroleptics mutually inhibit the metabolism of each other.
Zuclopenthixol may reduce the effect of levodopa and the effect of adrenergic drugs.
Concomitant use of metoclopramide and piperazine increases the risk of extrapyramidal disorder/disturbances.
Since zuclopenthixol is partially metabolised by CYP2D6, concomitant use of drugs known to inhibit this enzyme may lead to decreased clearance of zuclopenthixol.
Increases in the QT interval related to antipsychotic treatment may be exacerbated by the co-administration of other drugs known to significantly prolong the QT interval. Co-administration of such drugs is not recommended and should be avoided (see Precautions). Relevant classes include: class Ia and III antiarrhythmics (e.g. quinidine, amiodarone, sotalol, dofetilide); certain antipsychotics (e.g. thioridazine); certain macrolides (e.g. erythromycin); certain antihistamines (e.g. terfenadine, astemizole); certain quinolone antibiotics (e.g. gatifloxacin, moxifloxacin).
The previously mentioned list is not exhaustive and other individual drugs known to significantly prolong QT interval (e.g. cisapride, lithium) should be avoided.
Drugs known to cause electrolyte disturbances such as thiazide diuretics (hypokalemia) and drugs known to increase the plasma concentration of zuclopenthixol should also be used with caution as they may increase the risk of QT prolongation and malignant arrhythmias (see Precautions).
Special precautions for disposal: Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: Zuclopenthixol decanoate may only be mixed with zuclopenthixol acetate, which is dissolved in the same oil.
Zuclopenthixol decanoate should not be mixed with modified-release formulations with sesame oil as the vehicle, since this would substantially alter the kinetics of the preparations involved.
Store below 25°C.
Keep the ampoules in the outer box in order to protect form light.
Shelf life: 3 years.
N05AF05 - zuclopenthixol ; Belongs to the class of thioxanthene derivatives antipsychotics.
Clopixol Depot soln for inj 200 mg/mL
10 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
